The difference between endotoxins and exotoxins
Written by Anina Werner · 31. October 2024
Some bacteria are toxic, meaning that they can cause harm by producing substances that are poisonous to other organisms. Classified as either endotoxins or exotoxins, these compounds play critical roles in bacterial infections. Endotoxins and exotoxins share few similarities, as they differ significantly in their structures, release mechanisms and effects on the immune system.
Table of contents
This article explains the key distinctions between endotoxins and exotoxins, and covers the various laboratory tests that clinicians can use to identify the specific bacterial species or strain causing an infection.
If you wish, you can also watch our video about endotoxins and exotoxins.
What is an endotoxin?
Endotoxins are biomolecules found in the outer membranes of Gram-negative bacteria, and are usually made up of lipopolysaccharides (LPS), which is why the terms ‘endotoxin’ and ‘LPS’ are often used interchangeably. These toxins are mainly released when bacteria die and undergo cell lysis, with only small amounts being released during bacterial growth and division.
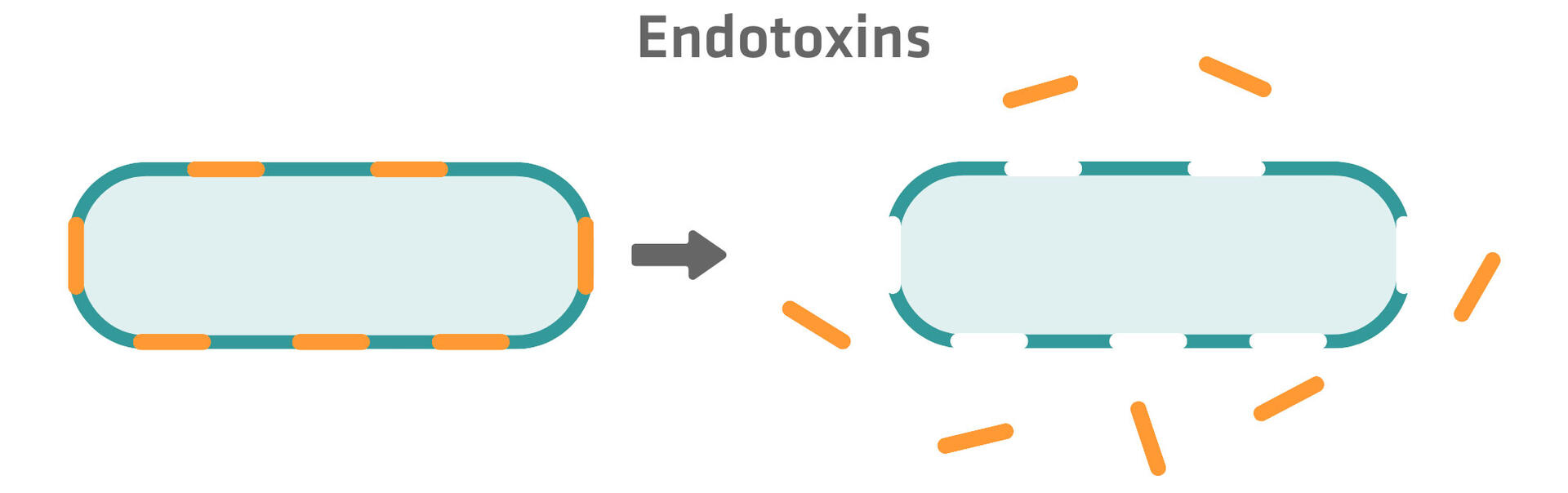
Structurally, endotoxins generally consist of a lipid A component, along with various sugar residues and phosphate groups. The lipid A portion is responsible for the toxic effects, but does not trigger antibody production, leaving hosts vulnerable to repeated infections and preventing the development of vaccines. Another characteristic of endotoxins is their heat stability, meaning that even autoclaved medical devices may not be completely free from them.
Endotoxins are non-specific in their effects on tissues, and can lead to Gram-negative sepsis and septic shock, which cause symptoms including fever, rapid breathing, fast heart rate, low blood pressure and, in severe cases, organ failure. Other common diseases caused by endotoxins are salmonellosis and tularemia. Examples of Gram-negative bacteria that produce endotoxins include Escherichia coli, Pseudomonas, Klebsiella, Salmonella and Francisella tularensis.
What is an exotoxin?
Exotoxins are proteins produced by many Gram-positive bacteria, as well as a few Gram-negative species. Unlike endotoxins, which are part of the outer bacterial membrane, exotoxins are produced as part of the bacteria's metabolic activity. They are constantly secreted into the extracellular environment or released during cell lysis.
Since exotoxins are proteins, they can be denatured by heat, meaning that properly cooked food is free of exotoxins. Another difference between exotoxins and endotoxins is that exotoxins are immunogenic. This means that they stimulate the immune system to produce antibodies, enabling the host to acquire immunity to exotoxins. However, certain exotoxins are so potent that they can cause significant harm – or even death – before the immune system can mount an effective response. The immunogenicity of exotoxins also opens the door for vaccine development. Vaccines against exotoxin diseases – such as tetanus – contain toxoids, which are modified versions of the toxins that are no longer harmful but still stimulate the immune system to produce antibodies.
Exotoxins are highly specific in their effects on tissues. Neurotoxins, for example, only act on tissues of the nervous system, where they can cause diseases like tetanus or botulism. Enterotoxins, in contrast, act on tissues of the gut, provoking conditions like cholera. Here is a list of common diseases caused by exotoxins:
- Toxic shock syndrome – caused by Staphylococcus aureus
- Tetanus – caused by Clostridium tetani
- Botulism – caused by Clostridium botulinum
- Gas gangrene – usually caused by Clostridium perfringens
- Diphtheria – usually caused by Corynebacterium diphtheriae
- Cholera – caused by Vibrio cholerae
- Staphylococcal food poisoning – caused by Staphylococcus aureus
Types of exotoxins
Exotoxins interact with specific receptors or biological mechanisms in the host, and can be classified into 3 main categories based on their mode of action.
Type 1
T4 lymphocytes are a type of white blood cell that limit and coordinate the immune response in case of an infection. They are normally only activated in low numbers, but certain type 1 exotoxins are superantigens that can bypass the normal activation process, activating up to 40 % of all T4 lymphocytes. This triggers the release of substances that can cause severe illnesses, including shock and multiorgan dysfunction.
Type 2
Type 2 exotoxins cause harm by forming pores in cell membranes, or by breaking down intracellular structures. This produces inflammation through direct action or the release of damage-associated molecular patterns (DAMPs). DAMPs released by damaged or infected cells can promote the spread of the infection into surrounding tissues or previously healthy areas.
Type 3
Type 3 exotoxins, known as A-B toxins, consist of 2 components: the active (A) component, which interferes with host cell functions, and the binding (B) component, which attaches to host cell receptors, determining which cells are affected.
Endotoxins vs exotoxins
This table provides a concise comparison of endotoxins and exotoxins, summarizing the key points discussed above for a quick overview.
| Endotoxins | Exotoxins | |
|---|---|---|
| Bacterial origin | Gram-negative bacteria | Many Gram-positive and a few Gram-negative bacteria |
| Chemical composition | Lipopolysaccharides | Proteins |
| Primary mode of release | Upon bacterial cell death | Secreted by living bacteria |
| Heat resistance | Heat stable | Heat labile |
| Immunogenic response | Poor antibody production | Strong antibody production |
| Effect on tissues | Non-specific | Highly specific |
| Examples of associated diseases | Gram-negative sepsis, septic shock, salmonellosis, tularemia | Toxic shock syndrome, tetanus, botulism, gas gangrene, diphtheria, cholera, staphylococcal food poisoning |
| Example bacterial producers | E. coli, Pseudomonas, Klebsiella, Salmonella | S. aureus, C. tetani, C. botulinum, C. perfringens, C. diphtheriae, V. cholerae |
Tests for bacterial infections
Several toxins can produce similar symptoms in a patient, and so clinicians often rely on laboratory tests to identify the infectious bacteria. The specificity and time-to-result of these tests are critical to ensure that patients receive effective antimicrobial treatments, and to minimize the use of broad-spectrum antibiotics that can accelerate the development of antibiotic-resistant bacteria. In this section, we will discuss the various laboratory tests available for detecting bacterial infections.
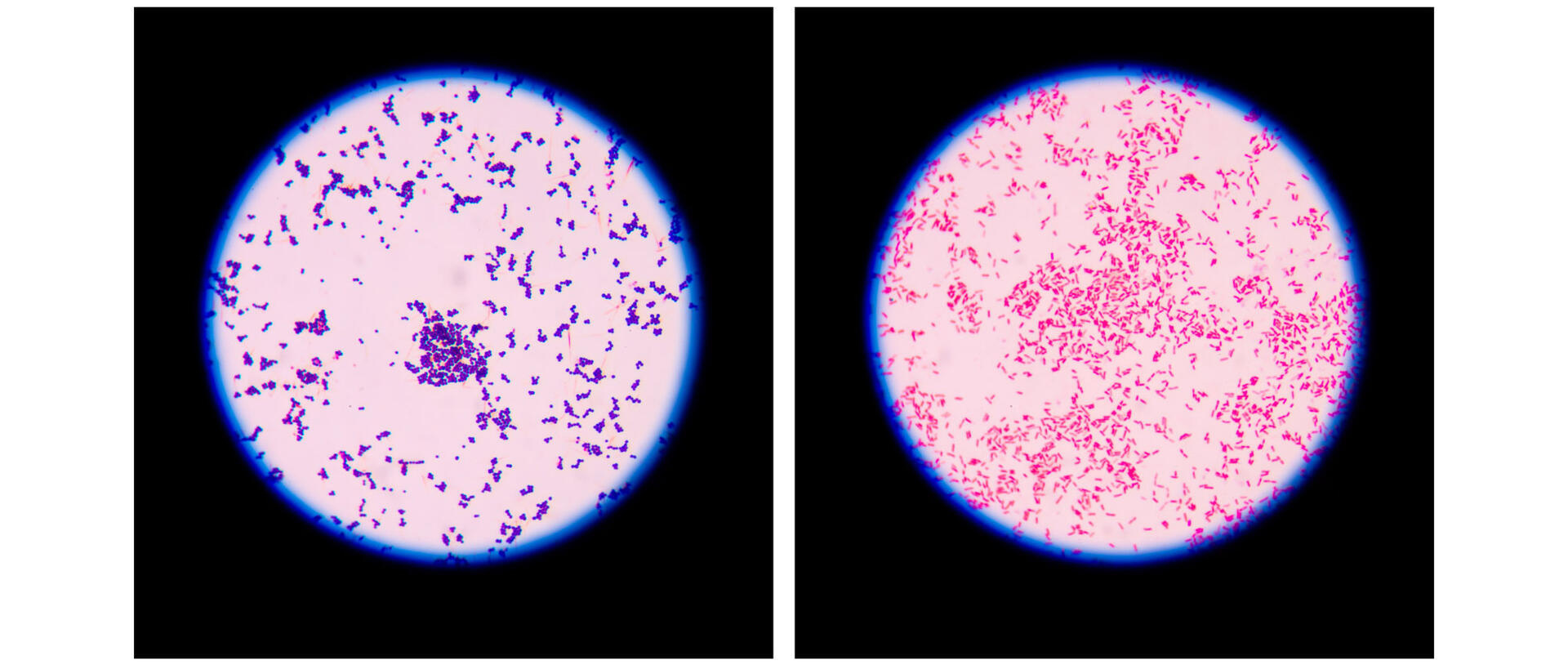
Microscopy
Microscopy is the easiest and fastest method to examine patient samples. Typically, the samples are stained before being viewed under a microscope. Various stains are available, and the choice depends on the suspected pathogen. For example, the most commonly used stain is the crystal violet Gram stain; Gram-positive bacteria retain it and appear blue, while Gram-negative bacteria do not, showing up as red. Such findings can help guide initial antibiotic therapy, but further tests are generally performed to precisely identify the pathogen.
Bacterial culture
Samples often don't contain enough bacterial cells to identify them under a microscope or by using other tests. One option to multiply the number of the bacterial cells in a sample is to grow them on or in a nutritional medium. The type of medium chosen and culture conditions, such as the temperature or oxygen concentration, are adapted based on the pathogen suspected. Bacterial cultures can then either be used to directly identify the pathogen present – for example, based on colony size, color and shape – or undergo further testing, such as chromatography or mass spectrometry.
Some exotoxins function as enzymes, such as hemolysin, which is produced by some Streptococci and Staphylococci species and lyses red blood cells. Culturing on blood agar can help to differentiate between species that lyse the cells completely (β-hemolysis), partially (α-hemolysis) or not at all (γ-hemolysis).

To learn more about bacterial cultures, please read our article How to culture bacteria.
Antimicrobial susceptibility testing
Bacterial cultures are often used for antimicrobial susceptibility tests. Bacteria can develop antibiotic resistance mechanisms and pass them on via horizontal gene transfer, which means that simply identifying the infectious pathogen is often insufficient. Clinicians also need to determine whether the bacteria in a patient's sample are still susceptible to the antibiotics they intend to prescribe.
Various culture-based tests to determine the susceptibility and sensitivity of bacteria to antibiotics are available, including agar dilution, broth dilution, antimicrobial gradient or disk diffusion. More information on how these techniques work can be found in our article Antimicrobial susceptibility tests: A comprehensive review of the most commonly used methods.
Genetic methods – such as PCR amplification followed by gel electrophoresis – can also be used to detect resistance mechanisms, and are particularly useful if there is no time to culture bacteria, or if the suspected pathogen is particularly slow growing or difficult to cultivate. However, genetic methods only identify known resistance genes, meaning that other, unidentified resistance mutations may still be present. The absence of known resistance genes therefore does not guarantee susceptibility. As a result, culture-based methods are usually preferred over genetic methods, despite taking longer to complete.
Genetic tests
In addition to antimicrobial susceptibility testing, genetic tests are also useful tools for detecting the specific bacterial species causing an infection. For instance, qualitative and quantitative PCR-based techniques, can be used to test for known suspected pathogens, and shotgun metagenomics sequencing allows the identification of all the species of bacteria present in a sample.
Immunogenic tests
Immunogenic tests can also allow the identification of bacteria present in samples that cannot be cultured, such as when the patient needs to be treated immediately or the suspected pathogen is unculturable. Immunogenic tests can either detect antigens produced by bacteria, or the antibodies produced by the patient's immune system in response to the bacterial infection. Commonly used immunogenic tests include:
- Agglutination tests: Agglutination tests involve coupling small particles to an antigen or antibody. When these particles are mixed with a sample, the presence of the target antibody or antigen causes the particles to cross-link, resulting in visible agglutination.
- Enzyme-linked immunosorbent assays (ELISAs): In ELISA tests, an antigen-antibody complex is immobilized to a solid surface. As an enzyme is attached to one of the molecules in the complex, the subsequent addition of an enzyme-specific substrate results in a colored reaction product, allowing the detection and quantification of the antigens or antibodies present. Learn more about ELISAs.
- Western blots: In western blots, the proteins in the sample are first denatured and separated by size. They are then transferred to a membrane, and specific antibodies are used to detect the antigens of interest. Results can be visualized using colorimetric, chemiluminescence or fluorescence analysis. Learn more about western blots.
Conclusion
In summary, knowing the difference between endotoxins and exotoxins, and identifying the exact bacterial species or strain responsible for an infection, are essential for accurate diagnosis and treatment. To ensure effective therapy, clinicians must also determine the bacterium’s antibiotic resistance. We hope this article has clarified the unique characteristics of each toxin type, their impacts on human health, and the various types of diagnostic tests available to clinicians. If you have any questions or comments, feel free to leave a message below.
Ask our expert. Leave a comment!
Write us if you have any questions regarding the blog article.